...
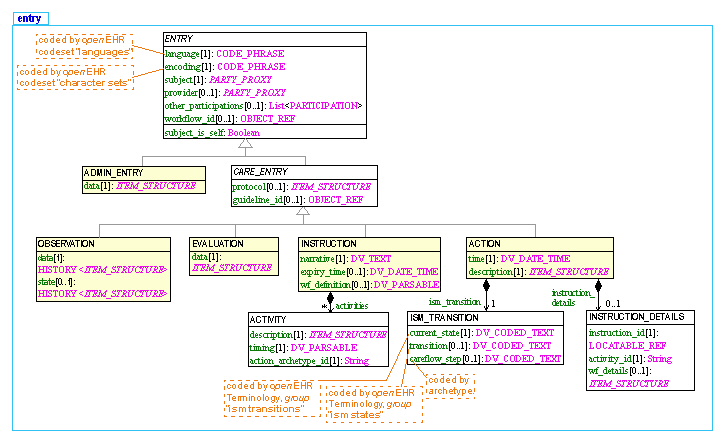
The openEHR Reference Model includes an information model which defines many classes. The information model, although relatively basic with respect to some of the ontologies in the biomedical space, nevertheless contains ontological commitments of its own - i.e. formal descriptions of certain real-world concepts relating to recorded health information. The part of the model of most ontological interest is the 'Entry' part, which is formally specified in the openEHR EHR Information Model; it can also be seen online as detailed UML. A summarised UML form of the Entry types in openEHR is illustrated below.
| There are 5 types of ENTRYs defined: an ADMIN_ENTRY type and 4 sorts of CARE_ENTRY types: OBSERVATION, EVALUATION, INSTRUCTION, and ACTION. The 6th type is called GENERIC_ENTRY, and is designed for mapping into and out of legacy and integration structures such as CEN EN13606, HL7 CDA, message and relational databases. The UML model of this type is here; it is documented in the openEHR Integration IM. All of these types are extremely generic and archetypes are used to define the specific business/domain content models under each of these types - see archetype mindmap for examples. |
The openEHR Entry model the way it is today has an ontological design which is described in a MedInfo 2007 paper. We can summarise the approach with the following three diagrams. The first is a model of process (shown in two ways); the second shows a cycle of information creation due to the process, and the last shows the information ontology developed in openEHR for recorded clinical
...
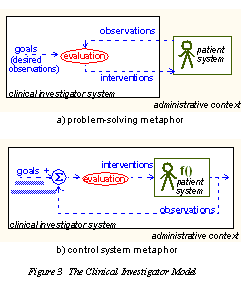
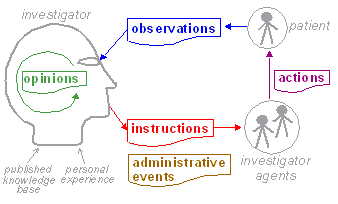
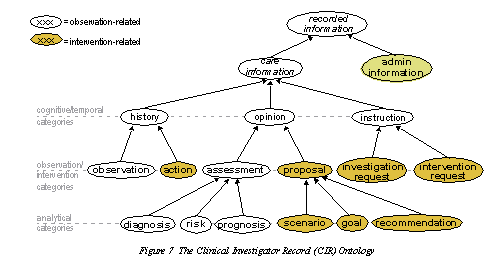
The explanation of the ontology behind the openEHR Entry model is in MedInfo 2007 paper. The following 3 diagrams show in a summarised way the ontological underpinning of the openEHR Entry model the way it is today. The first is a model of process, the second a model of information creation due to this process, and the third an ontology of information.
| We model health care delivery as two kinds of process: a clinical process, corresponding to the interaction between a 'clinical investigator system' and a 'patient system', situated within a business process, which is owned by an 'administrative context'. The clinical process constitutes a sub-process of the business process, i.e. it is the main mechanism for the business process to achieve its goal, which is to satisfy a demand for care on the part of the patient. The administrative context corresponds to the health system as a whole, rather than a single enterprise, since from the patient care point of view, the mobilisation of care delivery is carried out by a network of provider organisations. The model can be illustrated in two equivalent ways, as shown in Figure 3. |
| The terms 'observation', 'evaluation' etc defined above are not themselves the same as information types, since they refer to a variety of phenomena within the process: information from observations, the activity of evaluation, acts of intervention, and goal statements. To be more precise, we are mainly interested in information created by the investigator system, since this notional agent encompasses any person or device who/which performs any healthcare related task, including the patient herself. The investigator system is therefore the creator of all clinical information in the health record, including patient-entered data. A small amount of administrative information may also end up in the EHR, generally created by non-clinical actors in the organisational context.
|
| The Clinical Investigator Record (CIR) ontology: |
...