Proposal - Physical examination findings pattern
Background
The foundation considerations for establishing a common pattern to record physical examination findings were outlined in Heather Leslie's 2015 blog posts - Fractal exam findings I and Fractal exam findings II.
Essentially, these principles are:
There will never be only one, single way to record any clinical record, but clinical examination seems to be an extreme example where we require a robust semantic foundation with strong governance, that can then be expressed in a flexible, mix’n’match approach to be able to cater for each of the differing requirements identified above.
- Different health professionals record the same clinical concepts to different levels of detail or granularity;
- Different clinical purposes or contexts require recording of the same clinical concepts to different levels of detail or granularity; and
- Each of the above statements is further compounded by the individual, clinician-to-clinician variation within the same profession, clinical context or purpose.
In response to these fundamental requirements, we adopted a modelling pattern comprising a single OBSERVATION archetype in which multiple CLUSTERs for detailed exam findings can be nested to allow for the 'mix and match' approach required to cater for clinical diversity .
As of Feb 2019, we have a published Physical examination findings OBSERVATION archetype (OBSERVATION.exam). In practice it is little more than an ENTRY framework that allows modellers to nest the CLUSTER archetypes that represent their specific examination findings for their use case/dataset.
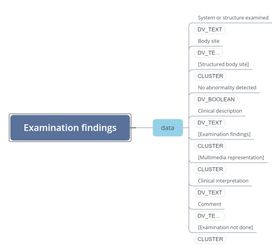
In parallel, we have agreed and published a generic Examination findings CLUSTER archetype (CLUSTER.exam). This is intended to be a generic foundation pattern for any type of detailed examination recording.
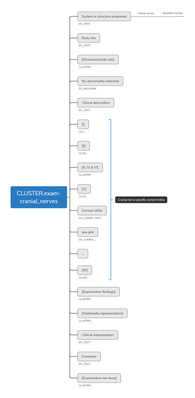
The intent is to develop specific archetypes for each examination finding. Yes, that will be a lot of archetypes, but probably not as many as you may first think.
The base pattern of the single OBSERVATION + multiple CLUSTER pattern appears sound and has withstood early implementations. Admittedly, these initial implementations have largely been fairly light on requirements for exam detail, and using SNOMED CT to define the 'System or structure examined' in the generic CLUSTER.exam has been adequate.
On the CKM today you will see the result of our first foray into building some of these specific exam-related archetypes, created over the past couple of years. Rightly or wrongly, they were each built as independent archetypes that effectively 'mirrored' the generic CLUSTER.exam, but in reality have no technical connection apart from an intent to have identical atcodes where possible. This choice was made largely because of the technical issues with managing specialisations of ADL 1.4 in the current tooling. But let's not get distracted by the pros and cons of ADL 1.4 vs 2.0 here because we have to resolve the issues only with the tooling we currently have at hand. And yes, despite best human efforts, the resulting archetypes do have some inconsistencies.While there are pros and cons with these archetypes as is, they have definitely demonstrated that the fractal patterns work well from a clinical documentation point of view. For example: Exam of both eyes > Exam of an eye > Exams of lens; retina etc. Also Exam of abdomen > Exam of uterus > Exam of fetus.
In summary, so far we have established the following as a forward path:
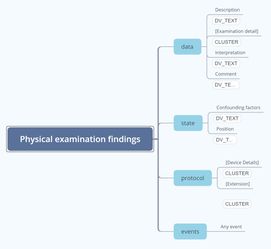
- Base clinical pattern consists of the 'Physical examination findings' OBSERVATION.exam nesting one to many CLUSTER.exam archetypes within the 'Examination detail' SLOT. Note: if the state of the patient changes, or a different devices are used, then this pattern may need to be represented for each state or device variation.
- Clinical pattern for the minimum generic content for the CLUSTER.exam, now agreed and published. SNOMED CT, or similar, bindings to be applied to the 'System or structure examined' data element where possible.
- Acknowledgement that we will need to create archetypes that capture additional detailed content that is specific for each examination.
We now feel confident that the pattern principle of a single OBSERVATION with our ability to mix and match various exam CLUSTERS will allow us to eventually represent the full scope of clinical examination. This is a significant discovery, and many thanks to all those who have been involved on that journey of discovery! Most people won't comprehend the amount of trial and error that underpinned the evolution of this pattern!
The current issue and proposed solution...
We are rapidly moving into a situation where we need to create archetypes that contain specific clinical examination content - this generic pattern is no longer enough.
Two options have been identified as a way to represent each exam specific finding:
- build specific CLUSTER archetypes for each exam finding, specialised from the generic Exam archetype despite the limitations of ADL1.4, that can carry the specific findings accurately;
OR
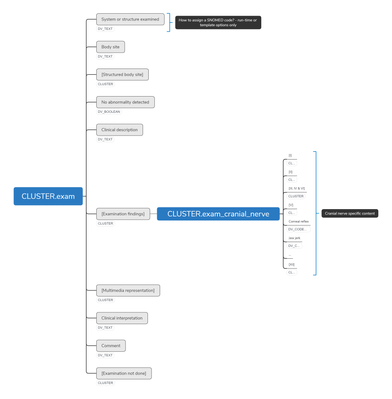
2. build CLUSTER archetypes for the specific content to be inserted into the 'Examination findings' SLOT within the generic CLUSTER.exam.
No matter which way we jump, either way we will need us to build an archetype per specific finding.
Some examples of use cases for the family of CLUSTER.exam specialisations are represented in the following files to further illustrate the modelling pattern intent:
{kind=link}
Based on our discussions with a limited group, we recommend the first option, but seek broader feedback.
In this modelling there is an inherent assumption that in most situations 'examination' refers to all modalities of physical examination applicable - ie any/all combinations of inspection, palpation, auscultation and/or percussion. This covers most clinical examination well - except where it doesn't!
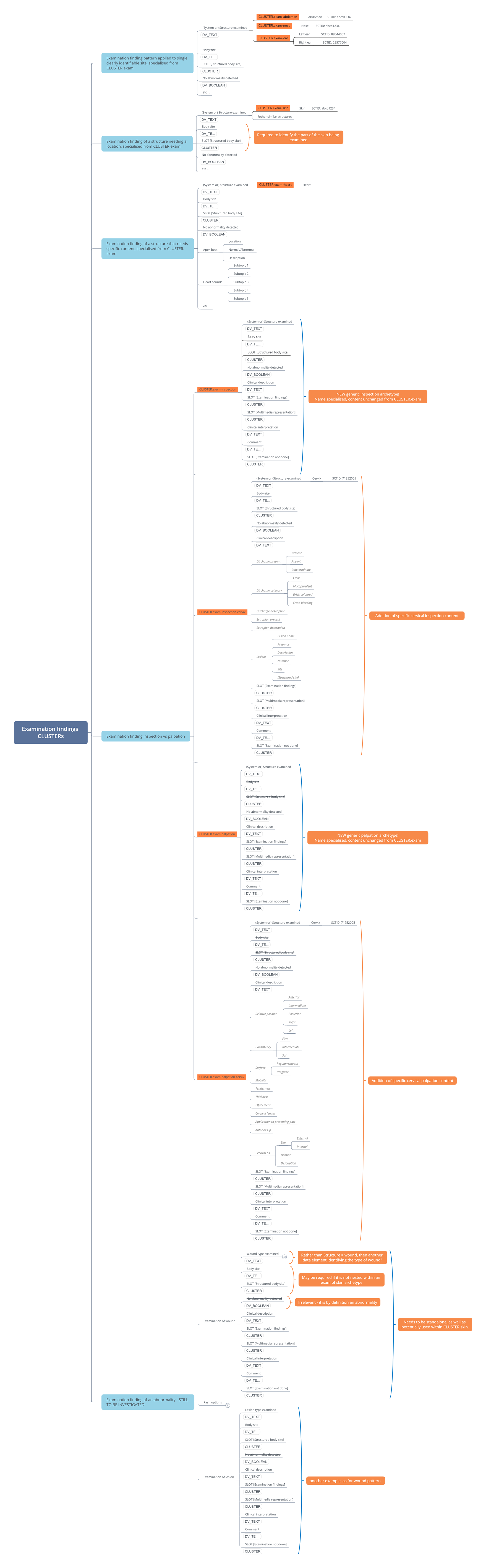
In response to implementer requests we have created some new archetypes to test the specialisation approach in recent weeks - Examination findings (CLUSTER.exam) has been specialised to create both a generic Inspection findings archetype (CLUSTER.exam-inspection) and a generic Palpation findings archetype (CLUSTER.exam-palpation), to support querying on a fairly limited number of examinations where Inspection or Palpation are the only methods used. The use cases that we have identified so far are limited to the vagina, cervix or rectum. For examination, recording inspection of any of these sites using a specific device. If the clinician also palpates these sites as part of examination, then they will usually do it using another instance of the OBSERVATION because of the change in device or patient state.
Otherwise it seems reasonable to assume that examinations usually consist of a combination of inspection, palpation etc. For example, percussion eg of chest or abdomen will usually not performed in isolation, so will most likely be recorded within a CLUSTER.exam specialisation
Please note that auscultation has been identified as having some unique requirements:
- We have not yet identified a use case for a generic auscultation archetype - CLUSTER.exam-auscultation - so at present we are not intending to create this archetype for future specialisation purposes.
- Auscultation of heart sounds will likely be modelled as part of the proposed CLUSTER.exam-heart as we have not identified a use case where this will be reused elsewhere or recorded in isolation to other types of heart examination.
- Archetypes for breath and abdominal sounds are specific use cases which will need to be represented as separate CLUSTERs so they can be re-used within either of CLUSTER.exam-chest and/or CLUSTER.exam-abdominal examinations. We haven't been able to identify any value in specialising them from a generic CLUSTER.exam-auscultation.
Please note that the only CLUSTER archetypes currently on CKM that represent this proposed pattern are CLUSTER.exam, CLUSTER.exam-inspection and CLUSTER.exam-palpation.
We would appreciate your feedback or questions for clarification
Mar 7, 2019