A three level model for registration of drug use and its potential benefits
When registering the drugs used by a person in an information system, especially if one want to use this data to obtain an overview of the actual medication status of a patient and/or to prevent for example drug interactions, one has to take into account that there are three levels of action involved.
The table below depicts these three levels and their sublevels.
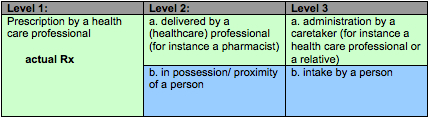
The first level is the actual prescription of a drug that is being registered.
This reflects the decision of a healthcare professional (for instance a doctor) to prescribe, based on a series of observations and/or evaluations, a drug to a patient/ citizen.
At best a level 1 registration provides an overview of all drugs prescribed to a patient/ citizen. This requires that all healthcare providers for that citizen have registered their prescription in such a manner that it can be used in a central information system. Unfortunately this ideal situation is still far away for most people.
Although it says nothing about the actual administration/ intake of a certain drug, registration of a prescription is (at least) required for medico legal purposes. Also it could for example have value to observe patient compliance. In the absence of other data it provides a good clue to the drugs that a patient/ citizen currently uses. Although thorough anamneses should reveal which drugs actually are being used and if there are other drugs that are being used.
The second level is the physical presence of a drug in the possession/ proximity of a person that is being registered.
Since one can look at this from two sides (delivery and reception) which both can be registered, we split level two into two sublevels.
a. delivery by a (healthcare) professional. This can be, and in case of a prescription drug will be a pharmacist. In the case of OTC/ non-prescription drugs this could for instance also be an employee of a drug store.
delivery by a (healthcare) professional. This can be, and in case of a prescription drug will be a pharmacist. In the case of OTC/ non-prescription drugs this could for instance also be an employee of a drug store.
drugs that have become into the possession and/or proximity of a person. For instance after reception of a prescription drug from a pharmacist or after purchase in a drug store. These are typically the drugs one has at home in a medication cabinet.
Registration of the delivery by a professional is required for at least administrative and often also for medico legal purposes.
In an ideal world all delivered drugs (both prescription and OTC drugs) are registered in such a manner that for every individual a complete overview is available to everyone who has permission to look at it.
Until then the registration (by the intended user) of the drugs in his/her medication cabinet could provide a good alternative. By doing so, at least of all the drugs available to a person are registered. Especially with regards to OTC drugs, food supplements and 'alternative' drugs this could provide a valuable oversight of all drugs available to a patient. Especially since these aren't registered otherwise. Such an overview could induce additional questions from/ observations to a healthcare provider. Also such an oversight could point to interactions between OTC and prescription drugs and/ or the misuse of OTC drugs.
Although it could provide useful information, registrations at level two says nothing about the actual administration/ intake of a certain drug.
The third level is the actual administration to, or intake by a patient/ citizen that is being registered.
Registrations at this third level represent the actual drug use provided that a patient/ citizen and/or his caretaker register everything properly. In the absence of integral and interoperable information systems, that are used by every healthcare professional and caretaker, self-registered drug use by the patient could provide the closest representation of the actual situation. Especially since it is that patient who benefits most of a good registration.
Level three self-registration of drug use will lead to many surprises for healthcare providers. It is for example well known that many people take drugs which where actually prescribed to a partner or another relative. For this fact alone self-registration of drugs could be of great value to prevent unnecessary side effects or interactions due to misuse.
In order to minimize registration errors during self-registration special requirements at input level are required.
Proposal to use a three level model for the registration of drug use
Since widely used integrated and semantic interoperable information systems are still years ahead of us, the clinical models used to register drug use should allow input on all three levels described above. Also it should allow both the entry of data by both the (healthcare) professionals who take care for as well as the patient/ citizen himself. Especially which regard to the so much debated 'patient empowerment' as well as the current developments known as health 2.0 it is unthinkable not to involve the subject of all these registrations: the patient/ citizen.
By allowing registration on all three levels of action (prescription, transfer and intake) and for the latter two, by having both the professionals and the patient/ citizen involved, the changes of obtaining an complete overview of the actual drug use increases tremendously. Furthermore, in the absence of an integral and interoperable information system, self-registration by the patient/ citizen is the best overview of the actual drug use one can obtain.
We therefore propose that the clinical model describing the uniform registration of drug use, takes into account the three level of action described above and allows registration by the patient/ citizen as well.
Version 1.0, November, 2008
S.F.F. (Stef) Verlinden.
